INTRODUCTION
Polycystic Ovary Syndrome (PCOS) is the hormonal imbalance in females, producing cyst in the ovaries and making it the leading cause of infertility in females. PCOS contributes towards 75% of female infertility.
REASON OF INFERTILITY IN PCOS
In females with PCOS, cyst formation does not allow the ovaries to release eggs. Due to this, the eggs become unable to fertilize with the sperms. When eggs are not released properly, the females also experience irregular menstrual cycles (anovulation). These irregular menstrual cycles are one of the major symptoms of PCOS.
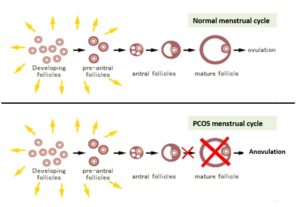
In normal menstrual cycle, a follicle (containing egg) is matured and becomes ready to ovulate. About 14 days after ovulation, menstrual period is expected if the female is not pregnant.
In PCOS, the follicle (antral follicle) with egg is unable to develop and mature due to which ovulation does not occur and results in irregular menstrual cycle.
Due to immature follicle, the egg becomes unable to fuse with sperm to conceive. Thus, infertility originates in PCOS suffering females.
High levels of insulin inside body interfere in the irregularity of menstrual cycle to develop anovulation and infertility. Insulin levels further stimulate the ovaries to produce androgens (testosterone), which also promote infertility. In most of the women with PCOS, the pituitary gland produces excessive amounts of luteinizing hormone (LH), which can stimulate the ovaries to secrete androgens. This further causes infertility in PCOS females.
CONTRIBUTION OF OBESITY IN PCOS TOWARDS INFERTILITY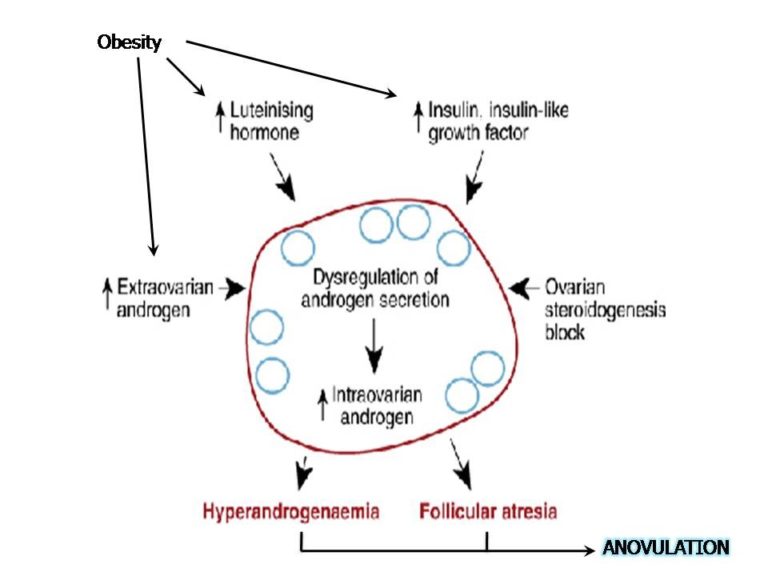
It is reported that obesity along with PCOS contributes majorly towards anovulation or infertility in women. The elevated levels of androgens and obesity lead to increased formation of estrogen hormone through insulin resistance. This hormone exerts a positive feedback on LH (luteinizing hormone) secretion and negative feedback on FSH (follicle-stimulating hormone) secretion. The increased levels of LH can lead to hyperplasia of the ovarian stroma and theca cells and increased ovarian androgen production (testosterones), which in turn provides more substrate for peripheral aromatization and be responsible for the chronic anovulation. Deregulation of FSH by testosterones interferes in normal follicle growth. Thus, follicle does not mature completely and results in anovulation.
TREATMENTS

Lifestyle modification: For overweight  women with PCOS who are anovulatory, diet adjustments and weight loss are associated with recommencement of spontaneous ovulation. One of the best ways to regulate the body weight and possibly reverse PCOS is through exercise and diet. It is considered as primary therapy for infertility in PCOS. Weight loss alone is associated with a reduction in serum-free testosterone concentration, which helps in ovulation and pregnancy. Weight reduction is also associated with management of insulin levels, which contributes towards reduction in symptoms of PCOS.
women with PCOS who are anovulatory, diet adjustments and weight loss are associated with recommencement of spontaneous ovulation. One of the best ways to regulate the body weight and possibly reverse PCOS is through exercise and diet. It is considered as primary therapy for infertility in PCOS. Weight loss alone is associated with a reduction in serum-free testosterone concentration, which helps in ovulation and pregnancy. Weight reduction is also associated with management of insulin levels, which contributes towards reduction in symptoms of PCOS.
Oral contraceptive pills: Oral contraceptive pills are reported to inhibit LH, diminish the circulating levels of androgens and increase the levels of circulating SHBG (sex-hormone binding globulin). It is advisable to use a low dose combination pill containing low dose of synthetic estrogen in combination with a low-androgenic progestin. These pills control menstrual cycles, reduce male hormones (testosterones) and help to clear acne also.
diminish the circulating levels of androgens and increase the levels of circulating SHBG (sex-hormone binding globulin). It is advisable to use a low dose combination pill containing low dose of synthetic estrogen in combination with a low-androgenic progestin. These pills control menstrual cycles, reduce male hormones (testosterones) and help to clear acne also.
Insulin sensitizing agents: Drugs initially  developed to treat type 2 diabetes have been used to treat PCOS. Some drugs improve insulin sensitivity by decreasing the circulating insulin levels. As these drugs do not enhance insulin production, therefore they are free from the risks of hypoglycaemia. Improving insulin sensitivity is associated with lowering testosterone levels which helps to improve ovulation rates.
developed to treat type 2 diabetes have been used to treat PCOS. Some drugs improve insulin sensitivity by decreasing the circulating insulin levels. As these drugs do not enhance insulin production, therefore they are free from the risks of hypoglycaemia. Improving insulin sensitivity is associated with lowering testosterone levels which helps to improve ovulation rates.
Fertility medications: Women with PCOS desirous of fertility are treated mostly for anovulatory infertility. Several medications that stimulate ovulation can help women with PCOS become pregnant. Treatment options include:
- Clomiphene citrate (CC) is the
 first line treatment in women with PCOS and anovulatory infertility. It causes increasing cervical mucus thickening and exhibits its anti-estrogenic effect on the endometrial lining; thereby negating any benefits of ovulation should it occur. On CC, the ovulation rate is around 70-80%. Clomiphene citrate is used early in the menstrual cycle to increase the chances of an egg being released by the ovary, which can then be fertilized naturally. It can be used either by itself or in combination with other drugs (e.g. insulin sensitisers) to increase its effectiveness.
first line treatment in women with PCOS and anovulatory infertility. It causes increasing cervical mucus thickening and exhibits its anti-estrogenic effect on the endometrial lining; thereby negating any benefits of ovulation should it occur. On CC, the ovulation rate is around 70-80%. Clomiphene citrate is used early in the menstrual cycle to increase the chances of an egg being released by the ovary, which can then be fertilized naturally. It can be used either by itself or in combination with other drugs (e.g. insulin sensitisers) to increase its effectiveness. - Letrozole (an aromatase inhibiter) is indicated as an effective agent for induction of ovulation in women with PCOS. This drug slows the estrogen production and causes the body to make more follicle-stimulating hormone (FSH), a hormone needed for ovulation. Letrozole is as effective as clomiphene in causing ovulation.
- Gonadotrophins are hormones involved in regulating ovulation by managing follicle-stimulating hormone (FSH), luteinising hormone (LH), human chorionic gonadotrophin (hCG). The medication is injected and the ovary carefully monitored by ultrasound to avoid over stimulation. These can also be used for treating infertility where women have not responded to clomiphene citrate.

Furocyst (fenugreek seed extract) treatment

It has been demonstrated by clinical studies that the bioactive components present in fenugreek seed extract – Furocyst contributes majorly towards the management of PCOS and induction of fertility. These bioactive components target insulin resistance to normalize the resultant overproduction of testosterones. It was also observed during the clinical study that Furocyst maintained regularity in menstrual cycle in PCOS women on completion of the treatment and women also got pregnant. It is known in PCOS that hormone levels such as luteinizing hormone (LH) and follicle stimulating hormone (FSH) levels are reduced which is also one of the reasons behind infertility. But Furocyst treatment showed significant increase in LH and FSH levels in the women. Thus, the study concluded that Furocyst was efficacious in ameliorating PCOS.
According to Chaudhary S et al., insulin resistance plays important role in the reproductive dysfunction in women. They reported that PCOS women have insulin resistance, which gives rise to infertility in them. According to their study, reduction in insulin resistance causes improved action of androgen on target tissues that offers the possibility of improvement in the physical stigmata of androgen excess leading to correction of the reproductive dysfunction and prevention of metabolic derangements. Fenugreek seed extract – Furocyst has been reported to target insulin resistance, which might contribute in the prevention of infertility in PCOS women.
In a randomized, double-blinded and placebo-controlled trial of fenugreek seed extract conducted by Bashtian MH et al., it was observed that fenugreek maintained the regularity in menstrual cycle in PCOS women. Pregnancies were also observed after the fenugreek seed extract treatment. They also showed that fenugreek had significantly positive effect on the insulin resistance.
Furocyst is an innovative product (extracted and developed through a novel & innovative U.S. patented process) involving separations of active ingredients from the natural plant without affecting chemical properties of the active fractions. No chemicals are used. It is a natural and promising dietary supplement for the management of Polycystic Ovary Syndrome (PCOS).
 REFERENCES
REFERENCES
- http://www.advancedfertility.com/pcos.htm
- https://jeanhailes.org.au/health-a-z/pcos/fertility-management-treatment
- https://www.nichd.nih.gov/health/topics/PCOS/conditioninfo/Pages/infertility.aspx
- http://202.120.143.134/Download/c250ac8a652942551493de542064-299708120125.pdf
- http://womenshealth.gov/publications/our-publications/fact-sheet/polycystic-ovary-syndrome.html
- https://www.arcfertility.com/polycystic-ovarian-syndrome-insulin-resistance/
- http://ijpr.sbmu.ac.ir/pdf_1296_3b0a5cb275247dc60c246cac1b579bda.html
- http://www.pmrc.org.pk/Insulin%20Resistance,PJMR-2012%20_2_,p63-65.pdf
- http://www.fasebj.org/content/29/1_Supplement/936.7?related-urls=yes&legid=fasebj;29/1_Supplement/936.7
- https://furocyst.com/